Answer:
Subdiaphragmatic Abscess
Findings:
Gas- Fluid Level below right dome of diaphragm.
Reactive right pleural effusion and right basal atelectasis.
Discussion:
Subdiaphragmatic abscess must be clinically suspected in patients with continuous fever post abdominal surgery.
One of the early evidences of subphrenic abscess is restricted mobility of the involved hemidiaphragm. This can be best demonstrated fluoroscopically. Elevation and fixation of the hemidiaphragm occur later. This change is more prominent and more readily evident on the right. Particular attention should be directed to the posterior aspect of the right hemidiaphragm. It normally slopes acutely caudad from its convexity. With abscess in the posterior suprahepatic space, this slope is reduced and may be completely eliminate. Ultrasound can demonstrate fluid collections easily, but when there is associated gas, the sonographic window will be very much reduced. CT with Contrast will confirm the diagnosis.
Subdiaphragmatic Abscess
Findings:
Gas- Fluid Level below right dome of diaphragm.
Reactive right pleural effusion and right basal atelectasis.
Discussion:
Subdiaphragmatic abscess must be clinically suspected in patients with continuous fever post abdominal surgery.
One of the early evidences of subphrenic abscess is restricted mobility of the involved hemidiaphragm. This can be best demonstrated fluoroscopically. Elevation and fixation of the hemidiaphragm occur later. This change is more prominent and more readily evident on the right. Particular attention should be directed to the posterior aspect of the right hemidiaphragm. It normally slopes acutely caudad from its convexity. With abscess in the posterior suprahepatic space, this slope is reduced and may be completely eliminate. Ultrasound can demonstrate fluid collections easily, but when there is associated gas, the sonographic window will be very much reduced. CT with Contrast will confirm the diagnosis.
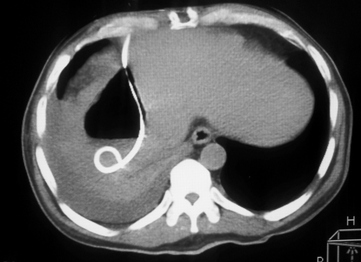
Percutaneous Pigtail Catheter Drainage of the Subdiaphragmatic Abscess